
CHRONIC PAIN, CHIROPRACTIC AND THE BRAIN, PART 4: HANDS-ON APPROACH
In this final installment of the series on chronic pain, I want to cover some of the modifications of hands-on manual therapy that may best address the unique central nervous system dysfunction associated with chronic pain. What may work for a more immediate issue, or episodically relapsing, with more of a peripheral and less of the central nervous system involvement may really backfire in chronic pain.
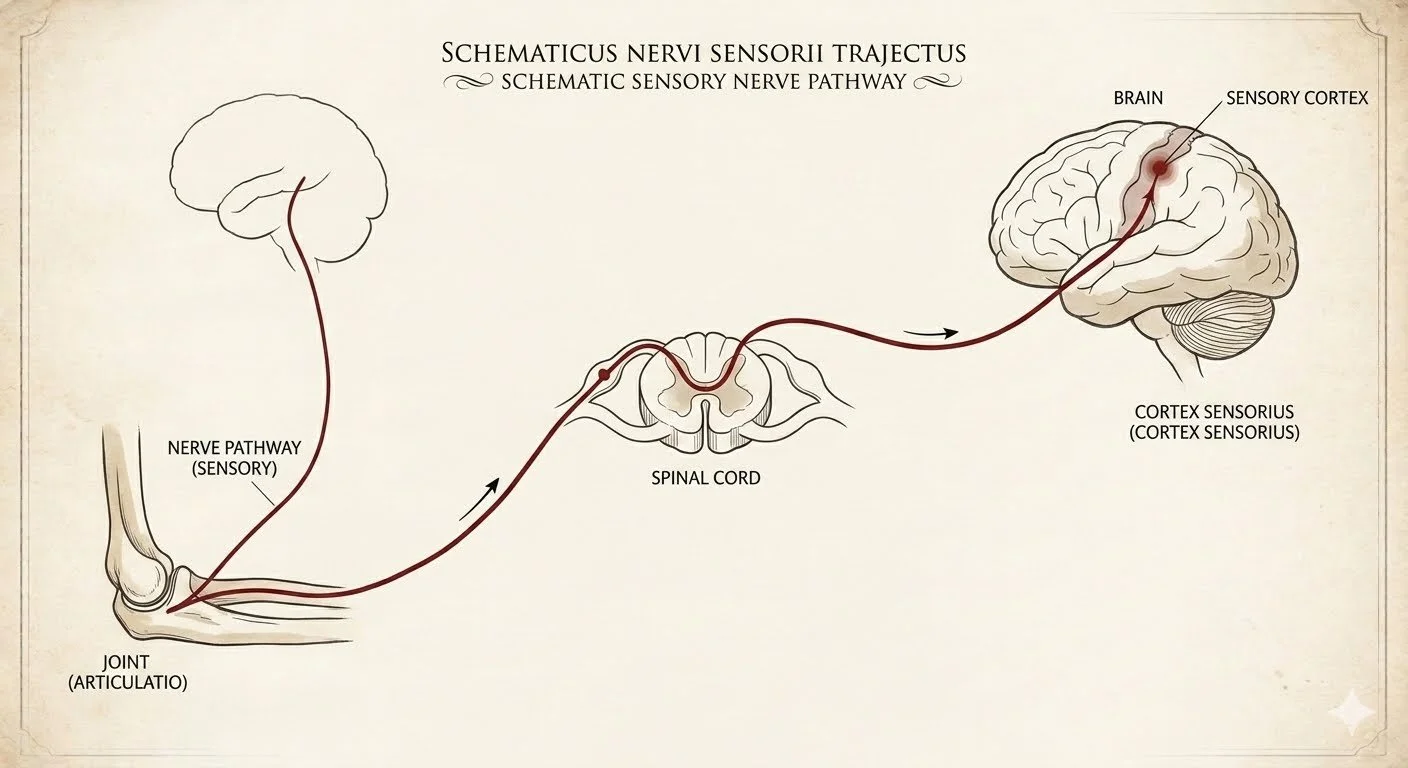
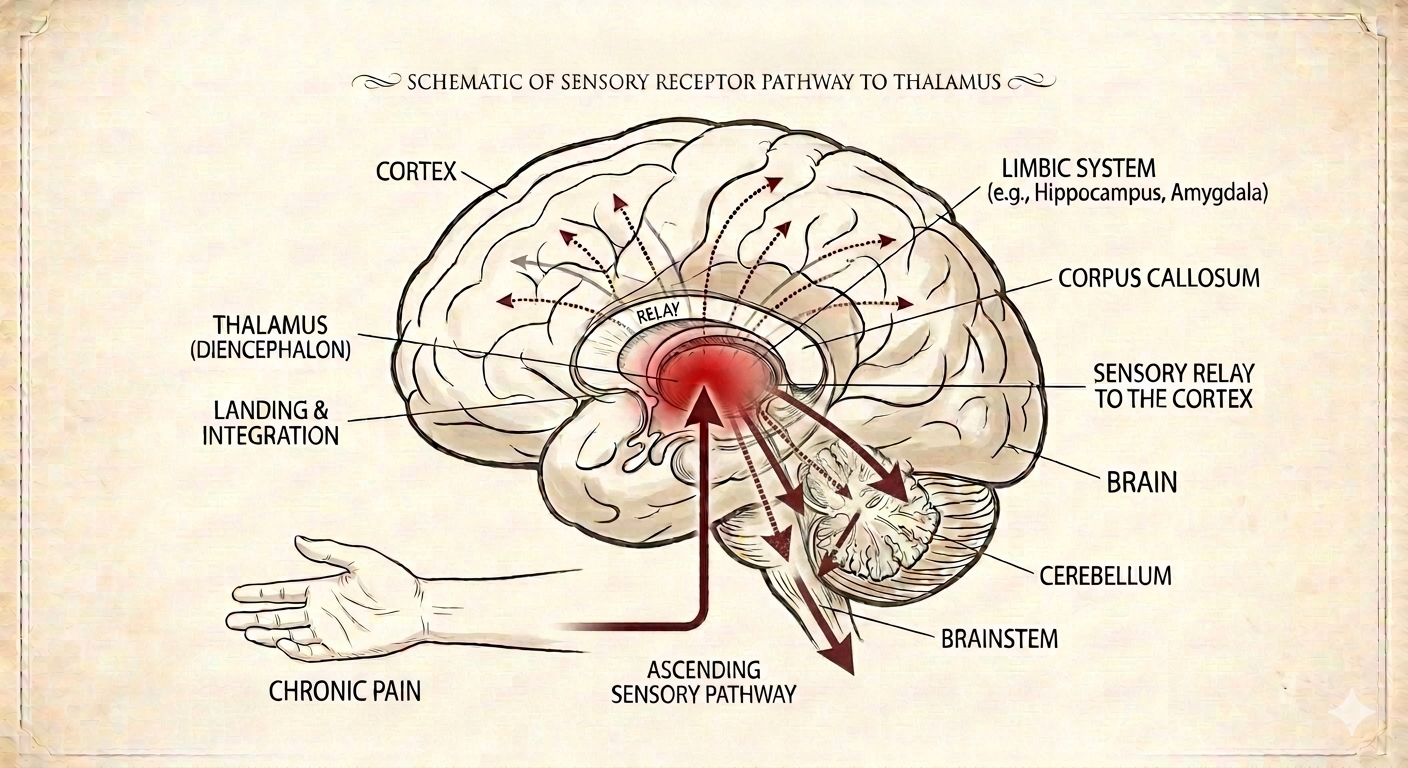
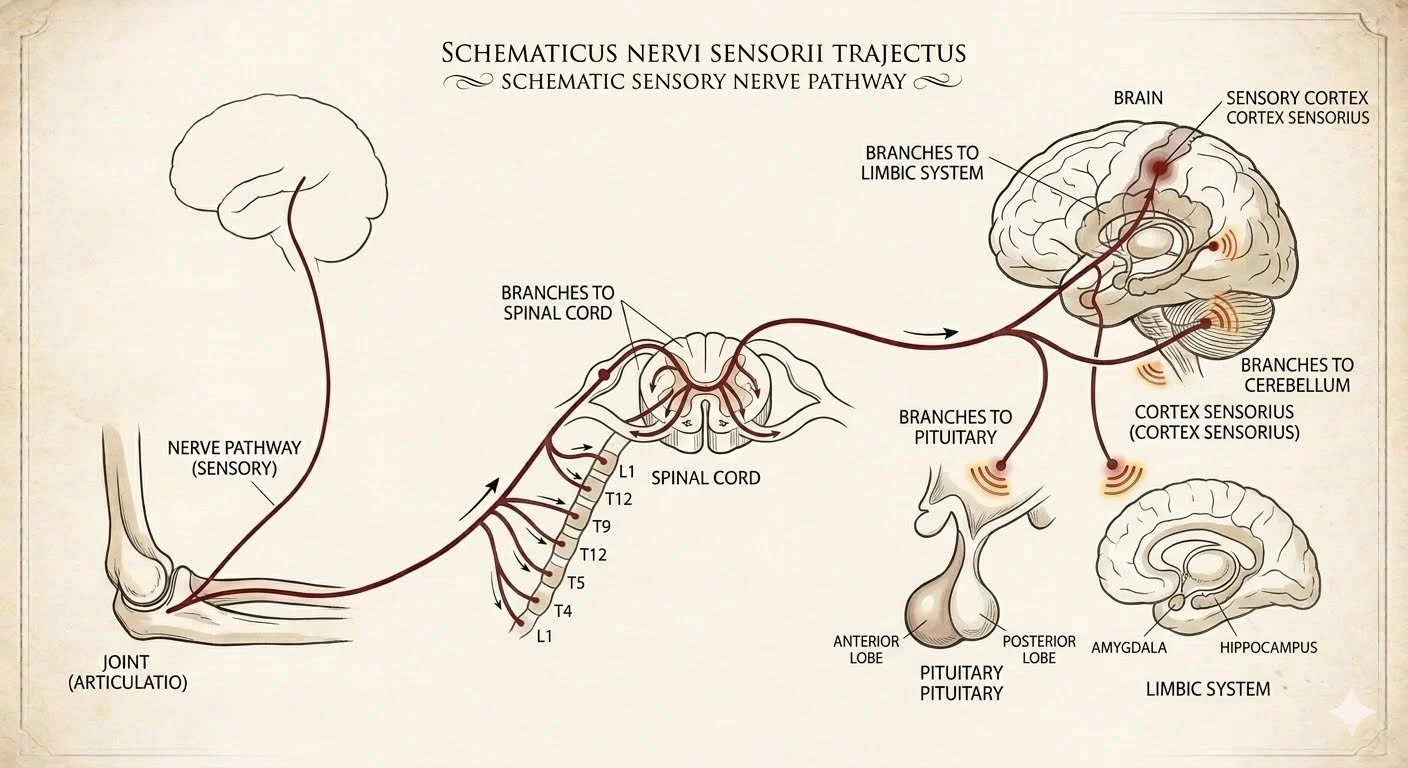
Since one of the hallmarks of chronic pain is the fact that pain signal is becoming very "efficient" and amplified and multiple points along the relay from the site of injury and the periphery through the spinal cord, and the sensory cortex, including all of the other branching off to other parts of the brain, manual therapy should avoid amplifying and that efficient pain transmission any further.
A fairly natural and instinctive reflex of people with chronic pain is to "dig deep" into the areas affected. If the sensory transmission loops in the sensory cortex perception of sensory transmission are working normally, that approach is going to be successful. However if the central nervous system is hyper sensitized to any sort of pressure on the affected peripheral tissues, the result will be counterproductive, with increased C pain fiber transition lighting up the cortex and feeding into the chronic pain cycle, making it even more "efficient", likely to fire up with less pressure at the next opportunity. At that point, that approach becomes nonbeneficial.
The way to address this self perpetuating and self amplifying positive feedback loop of chronic pain is to look at sensory input that competes rather than amplifies it. There are several ways to achieve that:
– 1st, look away from the proverbial bull's-eye. It means that sometimes, you do some therapy on an area outside of the targeted chronic pain area. It makes no sense to patient but from a neurological perspective, you are giving competition to the chronically hyper sensitized area by inputting normal signal from adjacent areas into the sensory cortex, efficiently reducing the amount of chronic pain C fibers reaching the sensory cortex and eliciting a perception of pain.
– Certain sensory input do not feed into the chronic amplifying C fiber pathways: light high-frequency vibration, extremely light sensory touch and brushing, mild heat. Using those therapies on and around the affected pain producing areas can also give competition to the sensory cortex, by retraining the brain to perceive sensory input from those areas rather than pain. While we use them in the office, these are the types of therapies that should be part of a home program, including very light high-frequency vibratory home device (something as simple as a high-frequency vibrating kids toy, or a handheld massager held very lightly on the skin at a high-frequency), light sensory brushing, gentle heat from either direct pad or infrared/red light therapy.
– Position sensors, such as those in joints, sensing in which direction joint is moving and how far, are also extremely good at down regulating chronic C fiber pain transmission. This is why instinctively a lot of patients with chronic pain will continue to rock, continuously move and try to rearrange or stretch the affected area. We can leverage that from a therapeutic standpoint by having patient doing active range of motion of an affected area, with in a pain free range, frequently.
There are unique challenges to healthcare providers like chiropractors and how to manually treat an area affected by chronic pain sensitization. 32 years into this great mighty a venture of patient care, I've come to realize that in the situation, "less is more". It means that I have to be realistic that achieving your musculoskeletal structural correction will require more time, less force, more precision and specificity, and respecting the body's ability to respond to my input without triggering an amplified pain response at the level of the brain. It also means that sometimes we have to communicate what we're doing and why would doing it in the we were doing it to patients, who legitimately expect that more is going to be better in this situation. It's also important to educate patients about how they handle the area at home. Shifting them from using deep pain producing, chronic C fiber pain perpetuating therapies to themselves (such as vigorous rolling, self massaging etc.) to things that are much more gentle and down regulating of the chronic pain cycle, including light brushing and vibration therapy at home.