





Reminder Due to the statewide mandate being put into place Saturday, July 25th, masks will be required for each appointment. Please plan accordingly. We will have additional masks available at the front desk if you forget one.

Chiropractic Beyond Pain Part 3: Dyskenia, Loss of Precise Movement
This blog entry should really have been written by Dr. Alvarez, but apparently I have dumped one too many administrative duties on her desk this week, so I will try to do it a wee bit of justice.
In the “beyond pain” series, I have discussed two aspect of spinal functional lesions (AKA subluxation in our technical jargon), that are not manifested as pain: loss of normal sensory perception and loss of normal energy expenditure resulting in fatigue. There are two more on the list and the next one is dyskinesia: the impairment of normal voluntary motor function.
Dyskinesia can be difficult to explain. People often think that we are talking about loss of strength, or loss of movement, but neither fully captures it. Dyskinesia is what happens when you want to accomplish a movement but the movement does not come out the way you want it: the range is not correct, the aim is not correct, the amount of force is too little or too much, or the movement itself is choppy instead of smooth.
Athletes instinctively know what dyskinesia is, even if they have never heard the word: when your pitching arm doesn’t release at the right time, when you overshoot your jump for example. Your brain circuitry has perfectly issued the command but the execution is distorted. You do not have to be an athlete to experience dyskinesia. Musicians are acutely aware of that problem when hitting the right key or the right string as well, and the “athletes of daily life” will see that manifestation when your intended muscle movement is rachety and inefficient, for example when typing or writing by hand.
One of my mentors in my last year of school was educating his patients about how to detect non-pain manifestation of their recurring spinal issues with an old fashioned fridge magnet (good marketing tool, he made some magnets with the office logo). He would have patients stand in front of the fridge, reach out with their index finger to touch the center of the magnet and repeat with their eyes closed. When they started to hit the outside of the magnet, it was time to schedule an appointment. I am pretty sure they had never heard of that word either, but they understood the correlation between spinal functional lesions and loss or motor efficiency.
https://www.researchgate.net/publication/320306138_Heart_Rate_Variability_to_Assess_the_Changes_in_Autonomic_Nervous_System_Function_Associated_With_Vertebral_Subluxation
0 Likes
SHOULDERS: PART 1- WHAT'S THE SCOOP?
The shoulder is made up of four joints. 1. Acromial-clavicular (AC), 2. Sternoclavicular (SC), 3. Glenohumeral (GH), 4. Scapulothoracic. The traditional main muscles of the shoulder include the SITS muscles or Supraspinatous, Infraspinatous, Teres Minor and Subscapularis. You can see where these muscles attach and their function based on the included image:

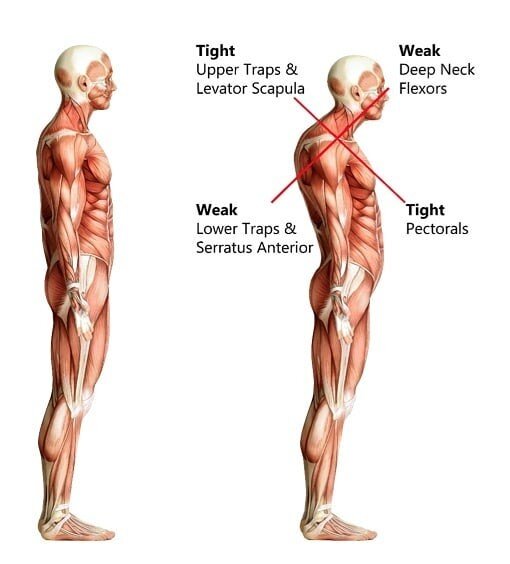
Poor posture usually due to poor working mechanics with desk jobs as well as this not so new world of looking down at cell phones can lead to what we call forward head carriage and then upper cross syndrome. The following image shows how upper cross syndrome can affect you.
Shoulder injuries are incredibly common in sport. Some include, but are certainly not limited to: Softball/Baseball (tendonitis, rotator cuff, SLAP tears), Hockey (shoulder separation & dislocation, clavicle fracture), Tennis (shoulder impingement, rotator cuff tendonitis, shoulder bursitis, sprains and/or strains), Volleyball (shoulder impingement and labral tears).
If shoulder injuries are so common in sport, how and what should we do to protect ourselves or our athletes and keep them performing at their best. First we need to begin with understanding the mobility stability continuum. Basically this is that every other joint is either needed for mobility or stability. Yes, there are specific areas throughout your body that you DO NOT want to be “mobile” but rather you want them to be stable in order to support the mobile areas.

Chiropractic Beyond Pain Part 2 : Dysponesis, Energy Management, Fatigue
After discussing the implication of spinal functional lesions on sensory mapping (dysaffenrentiation), Dr. Kent addresses a much lesser known aspect of nerve regulation called dysponesis. Dysponesis means abnormal management of energy expenditure, either not enough energy assigned for a task or wasted energy on another.
For most people thinking about energy expenditure, the idea of burning up too many calories AKA energy on a task sounds like a good deal, but from an evolutionary perspective, the production of energy uses up a lot of precious resources (food, digestive, and metabolic work), and your nervous system is supposed to evaluate energy needs and expand as little as possible for a particular task in order to preserve resources for other needs. To some extent, the reason that there are over 8 billions of us on the planet is because our nervous system get a high Energy Star rating. Conversely, the body also knows when to assign enough energy to a crucial task that will keep you alive (pregnancy, flight response).
The challenge in connecting the dots between spinal functional lesions we see in our day to day chiropractic practice and dysponesis is that the latter can be difficult to measure. Chiropractors of past generations had some rather interesting, albeit rudimentary tools: surface heat measurement devices for example. In the early 2000, surface EMG device were quite popular in many chiropractic practices because they were non-invasive, quick, and easy to use. The surface EMG device measure electrical activity of superficial muscles, mostly on either side of the spine in the intrinsic muscle groups, but sometime also along the extremity where you could see a lot of abnormal muscle tone and random contractions from a pinched sciatic nerve for example. There is good research of what a normal paraspinal muscle activity graph should look like at rest, and the difference from an EMG reading on the side of a hot cervical spinal misalignment is striking. Spinal muscles burn up a lot of fuel, so some of these areas of high activity of the EMG indicate some poor energy usage. It also means that the muscle group could fire excessively when it is not supposed to (spasm, tightness), or that it could fail to fully contract and protect your neck when jarred (instability, susceptibility to injury).
Even more fascinating to me, after 26 years in practice, is the correlation between fatigue and chiropractic lesions. There is local fatigue, such as patients reporting that their head feels suddenly too heavy to hold, or that a leg “ feels like lead “. Those symptoms have no good orthopedic explanation until you look at it as a manifestation of dysponesis. They often spontaneously resolve after a few adjustments. There is also more general fatigue. Patients with acute spine injuries often report feeling totally wiped out even through they are adequately resting. I used to think that the pain was the source of the fatigue, but I have seen enough patients who had pretty modest pain from a new injury with comparatively high fatigue symptoms to now recognize that the neurological dysregulation of energy expenditure probably plays a bigger role than recognized.
https://www.researchgate.net/publication/320306138_Heart_Rate_Variability_to_Assess_the_Changes_in_Autonomic_Nervous_System_Function_Associated_With_Vertebral_Subluxation
Ice baths or Nah?

As sports begin to pick back up again I have been asked a bit about ice baths. I have never heard of anyone actually enjoying a nice cold ice bath after a rigorous practice or long days of games. Sure enough there is even limited research supporting positive effects of using an ice bath as a recovery tool! Sweet, no more awful recovery baths, but if they are not a positive way of recovery, then what is?
The attached article suggests based on athlete perception that contrast therapy may be a better option, participating athletes perceive to be more relaxing and find it easier to rest and sleep post-game or training.
What are your favorite recovery tools?
https://journals.lww.com/nsca-jscr/Fulltext/2011/04000/A_Random_Control_Trial_of_Contrast_Baths_and_Ice.23.aspx
Chiropractic beyond pain: chiropractic lesions, dysafferentiation and the altered body map
I have recently downloaded and splurged on some new chiropractic basic science research podcasts that I listen to during my commute, a real nerd heaven. The author of the study, Dr. Kent, has been ahead of his time in our profession. His research has been focused on the basic neurology of chiropractic and how it affects health, body function, well beyond pain.
The article is heavy on basic science. It explores the ways in which mechanical lesions and malfunction in spinal joints disrupts feedback loops between the brain and the body. At any given time, your body is in a constant state of “homeodynamics”, constantly getting feedback from your external environment ( for ex how hot it is ), and your internal environment ( for ex how much food just landed on your stomach ) , and responding correctly ( increase sweating if your body temp is too hot or start to secrete stomach acid to digest your burger ).
One of the first manifestations of a disrupted feedback loop is a phenomenon referred to as dysafferentiation, a big word that describes an distorted sensory input from your body to your brain. Truly dysafferentiation can be caused by several things, but this article explored the role of the spine mechanical lesions because of their prevalence. If you want a simpler image : your brain needs to have an accurate “map” of what is happening in your body in order to produce the right response. Dysafferentiation is basically a faulty, distorted map. ( excuse my nerdy old love of classic literature, but I could not resist the analogy to the Dorian Gray story ).
The connection between chiropractic care and dysafferentiation is that reducing the mechanical lesion at the spine can prevent the distortion of sensory input reaching the brain, and thus an incorrect response. This phenomenon can happen regardless of the presence or absence of pain, and regardless of what part of the body map is distorted. Think about what happens if your body decides not to sweat in 90’ weather or if your body refuses to produce digestive juices to break down that big fat burger…
https://www.researchgate.net/publication/320306138_Heart_Rate_Variability_to_Assess_the_Changes_in_Autonomic_Nervous_System_Function_Associated_With_Vertebral_Subluxation
My IT Band is tight. Not likely.
I tend to hear over and over again, “my IT band is too tight, I foam roll it all the time, but it just doesn’t seem to get better”. Well, chances are it’s not your IT band that is tight, but instead the tensor fasciae latae (TFL) muscle or the gluteus maximus muscle that is inserting into the IT band and even the TFL or Glut Max might not be “tight” but functioning inappropriately. So you can spend all your time targeting the wrong area and never really make much progress, but it hurts when you do it so it must be right, right? No. Victims vs Villains. What is the villain or causing the problem and what is just a symptom, casualty or victim of the problem?
The IT band is actually layers and layers of fascial tissue, fascial tissue differs from muscular tissue by the fibers that make them up and their vascularity.
So next time you go to foam roll your “tight IT band” try rolling the TFL or Gluteus Maximus muscles, or stop in and we can assess the villains.
The Not-So-Strange Exercise of Walking Backwards
https://www.youtube.com/watch?v=cslOAA3o5L8
One of the biggest challenges with the postural distortions of modern humans is that all of our activities are in front of us and below eye level. Over time this will cause a strong tendency for the body to lose its proper relationship to gravity and for the whole body to lean forward: the pelvis anterior to the heels, the shoulders anterior to the pelvis, and the head anterior to the shoulders. Holding all of these body areas at a leverage angle to the supporting structure below causes chronic painful muscle overload and difformity of the supporting ligaments and mechanical overload of several key structures like the front of the knees, and the spinal discs.
Preventing and reversing forward postural shift can take many forms. Limiting poor ergonomics such as elevating our reading material to eye level is one strategy, but modern life also requires us to actively practice activities that reset our brain’s response to gravity and makes us actively reset our whole body over our heels, 2 or 3 inches back from where we typically stand.
There are a variety of such practices: yoga, tai chi for example and an often forgotten and easy activity is also walking backwards.
Walking backwards fires up the same cerebellar brain pathways that make you better sense that you are leaning forward as well as fires up the muscle groups that pull you back up from your forward posture. It can be done pretty much anywhere with no equipment, and you don’t have to do it very long or very far to get the neurological benefits, however there are a couple of important caveats for safety and efficiency-
SAFETY: Always check behind you to make sure that you have a clear path for the distance you are going to walk back. That seems like a no-brainer but from what I have seen at the office, not always the case… If you walk with a buddy for exercise you can have your partner be a spotter while you do this for a couple of minutes.
EFFICIENCY: Start by making sure you are standing tall and relaxed. Also YOU ALWAYS NEED TO SWING YOUR ARMS while walking backwards to get the neurological benefits. You will be surprised that it will take you a little bit of intention to find the correct arm to opposite leg coordination at first. This is why I do not recommend walking backwards while holding on to a wall, since you will be preventing normal arm swing. I also advise patients to only walk backwards on the treadmill if they can do it without holding on the the handrails.
