

In this section I would like to review some important concepts on how we treat chronic pain differently than acute pain, with the understanding that this is a vast complex and evolving field, and we will only be able to touch on the surface in this blog entry. In this section I will focus on how we understand the brain's reaction to chronic pain, while focusing on how we need to modify body care approaches in the following section.
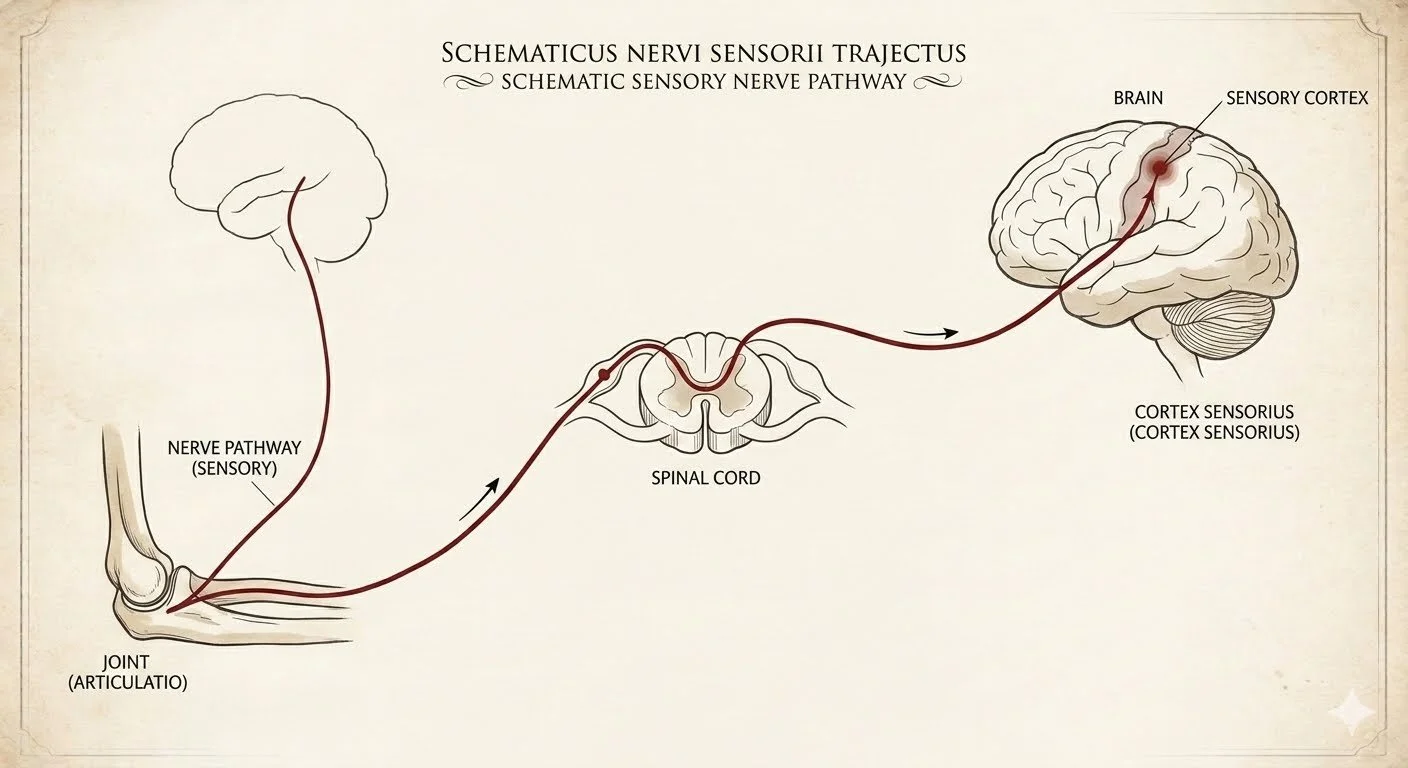
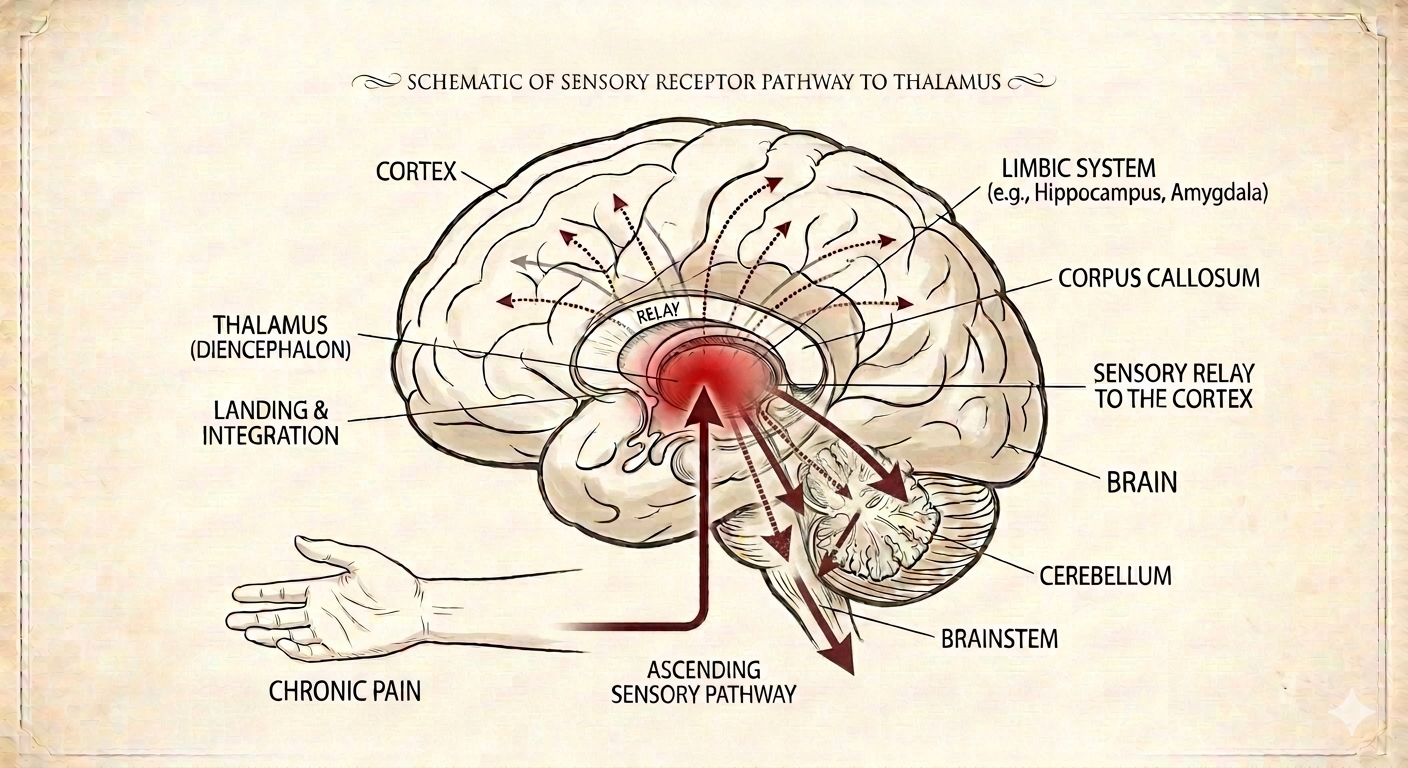
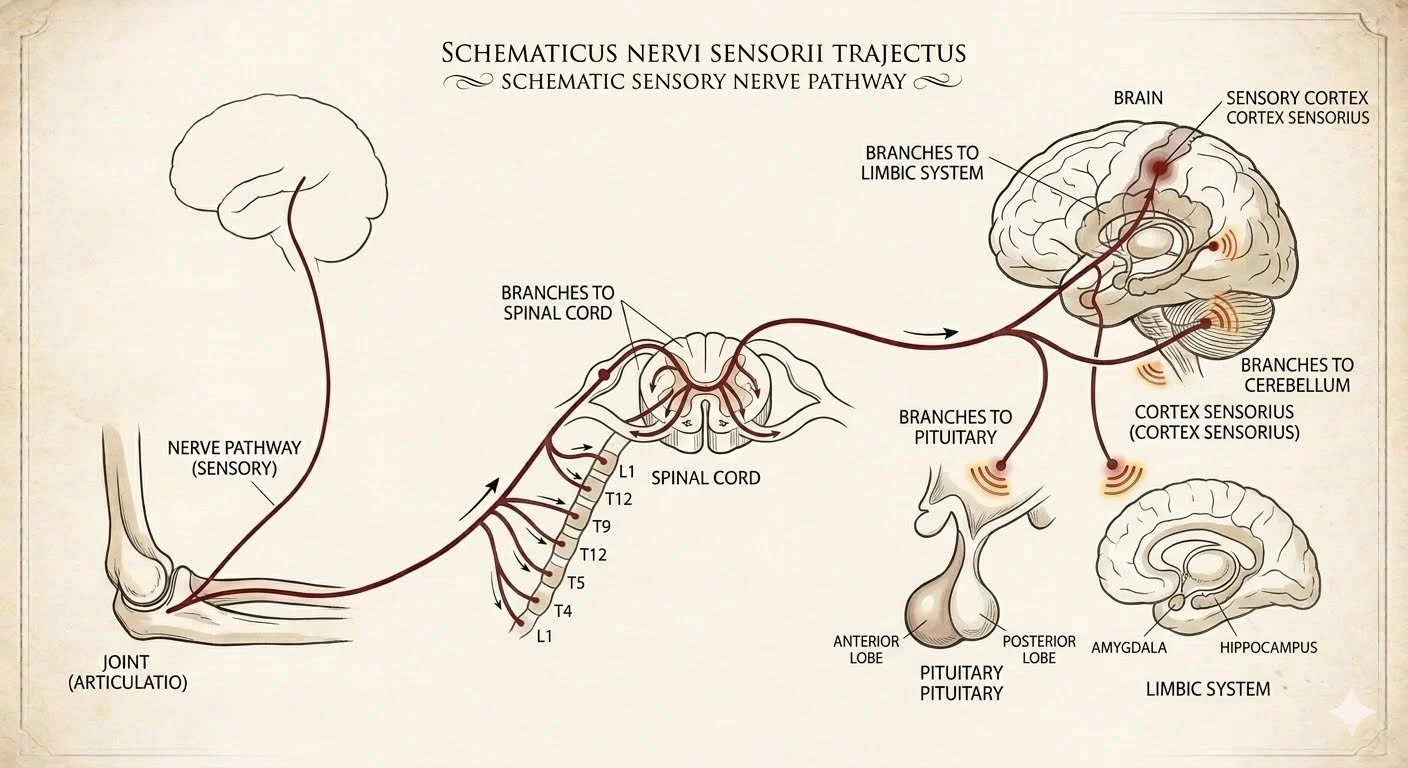
In section 2 we discussed how chronic pain is transmitted differently and more "efficiently" to the brain, with much more signal ramification into other parts of the brain as well. Meaning that chronic pain can be triggered with minimal sensory input, and is more perpetuated and activated at the level of the brain itself by other functions and parts of the brain. As a result, you really need to think about how well all of your brain is functioning when you're trying to manage chronic pain.
Brain nutrition and biochemistry: this is often overlooked in chronic pain. Making sure that the "chemical soup" of the brain is optimized to minimize inflammation, nutritional insufficiencies. Some low hanging fruit to improve your brain's response to chronic pain would be making sure that you stay away from oxidized fats (pretty much all refined seed oils of modern processed foods like sunflower oil, safflower oil, canola oil, etc.), focusing on whole foods complex fat and essential fatty acid from the fish and seafood family. Making sure you have adequate amounts of protein, optimizing vitamin D levels, electrolytes such as potassium and magnesium especially (involved in brain energy production and sustenance), minimizing blood sugar fluctuations by staying away from refined carbohydrates, making sure you have adequate amount of whole foods antioxidants, and staying away from ultra processed food since most of these food additives are known to be excitatory and inflammatory to the brain.
Of special note is a nutrient that we often do not think of as such for the brain which is oxygen. Chronic pain can often be associated with down regulation of the autonomic vascular system, meaning that we tend to have decreased blood flow perfusion to all parts of our bodies but especially to the central nervous system. Mild regular cardiovascular aerobic activity that gets your heart rate above 100 is really important in that regard, as is basic breath works. Making sure you don't have chronic low-grade anemia, or reduced oxygen availability from smoking and vaping for example. Patients taking certain medications that are associated with decreased blood flow to the central nervous system will need to discuss the specifics on how best to mitigate those problem with the individual provider.
Stress: the physiological impact of stress on the brain is widespread and underestimated when it comes to chronic pain. But there's almost a 1:1 correlation between stress increase and chronic pain increase, so you really never are going to manage one without managing the other. It will look differently in individual people. Sometimes we need to 1st take a stock of the stress and look at practical strategies so that we can start making some cuts, while concurrently increasing patients coping resources towards the inevitable stress burden of real life.
Sleep: suboptimal sleep is also almost a 1:1 driver of poor chronic pain management and resolution. It's also a self-perpetuating vicious cycle since chronic pain tends to disrupt sleep, and poor sleep tends to worsen chronic pain. It's also important to realize that most people will easily reach for heavy-duty pharmacological interventions for sleep disruption, (not only medication but things like over-the-counter antihistamines, CBD/THC, melatonin etc.), which may backfire because of suppressing normal brain adaptative mechanism over time. It's surprising to me how many people still practice poor sleep hygiene in spite of widespread data available from Dr. Google, (simple things such reducing your screen exposure in the evening is still very hard to achieve for most people). So as a starting place, you may want to take a simple inventory of your sleep hygiene habits and start making some changes. Other changes such as sleeping positions, mattresses, temperature, supplementation may need to be individualized with your healthcare provider. I have found it helpful to look at tracking device for overall sleep quality when making changes, to make sure that you focusing your efforts on things that actually pay off for you.