



https://www.youtube.com/watch?v=cslOAA3o5L8
One of the biggest challenges with the postural distortions of modern humans is that all of our activities are in front of us and below eye level. Over time this will cause a strong tendency for the body to lose its proper relationship to gravity and for the whole body to lean forward: the pelvis anterior to the heels, the shoulders anterior to the pelvis, and the head anterior to the shoulders. Holding all of these body areas at a leverage angle to the supporting structure below causes chronic painful muscle overload and difformity of the supporting ligaments and mechanical overload of several key structures like the front of the knees, and the spinal discs.
Preventing and reversing forward postural shift can take many forms. Limiting poor ergonomics such as elevating our reading material to eye level is one strategy, but modern life also requires us to actively practice activities that reset our brain’s response to gravity and makes us actively reset our whole body over our heels, 2 or 3 inches back from where we typically stand.
There are a variety of such practices: yoga, tai chi for example and an often forgotten and easy activity is also walking backwards.
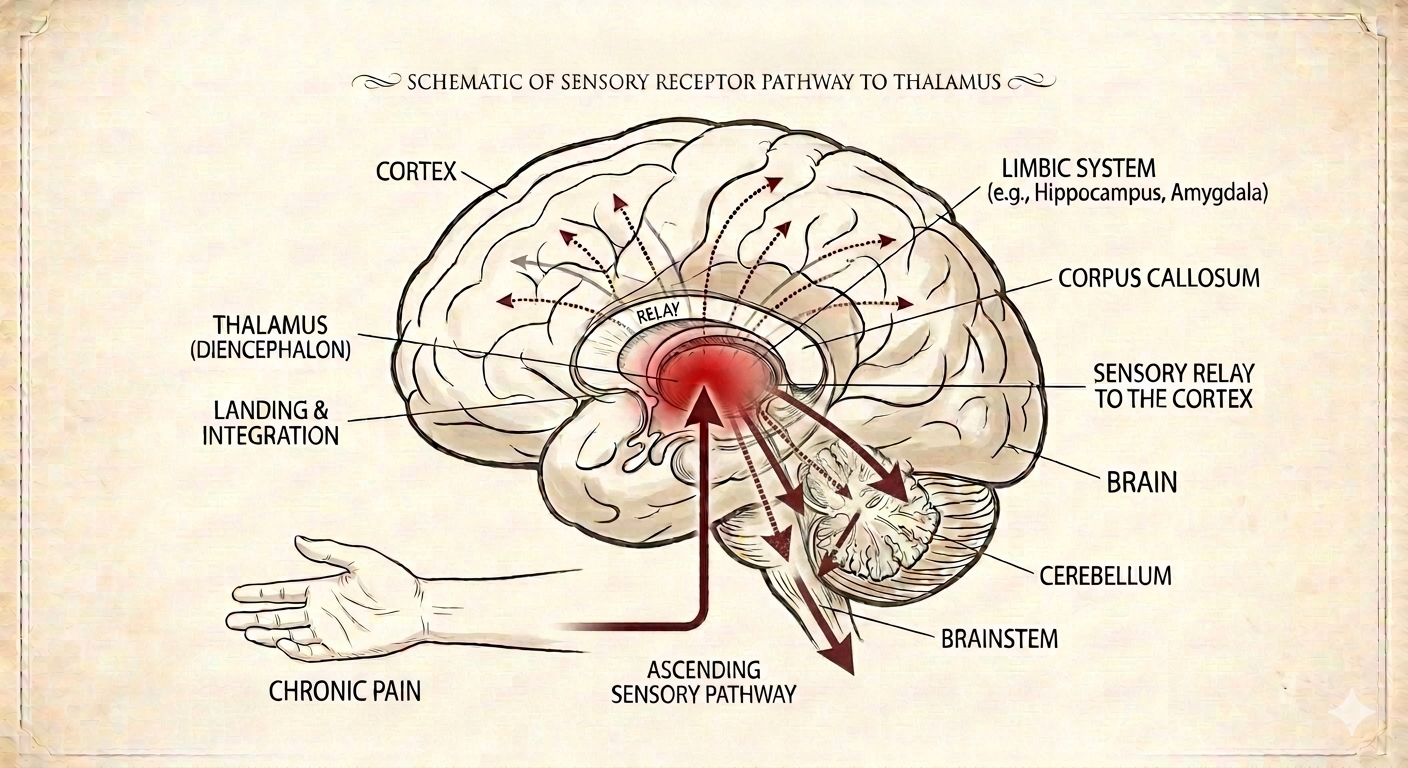
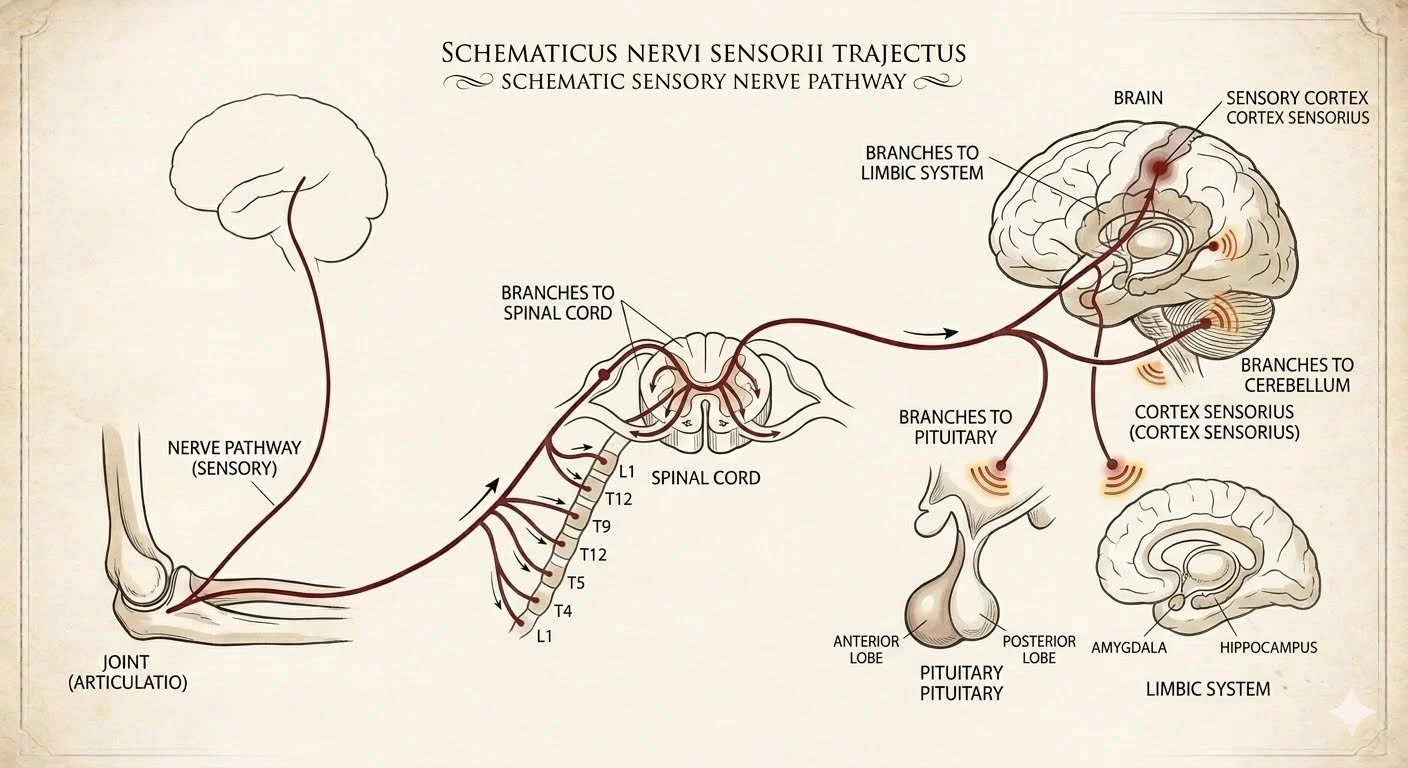
Walking backwards fires up the same cerebellar brain pathways that make you better sense that you are leaning forward as well as fires up the muscle groups that pull you back up from your forward posture. It can be done pretty much anywhere with no equipment, and you don’t have to do it very long or very far to get the neurological benefits, however there are a couple of important caveats for safety and efficiency-
SAFETY: Always check behind you to make sure that you have a clear path for the distance you are going to walk back. That seems like a no-brainer but from what I have seen at the office, not always the case… If you walk with a buddy for exercise you can have your partner be a spotter while you do this for a couple of minutes.
EFFICIENCY: Start by making sure you are standing tall and relaxed. Also YOU ALWAYS NEED TO SWING YOUR ARMS while walking backwards to get the neurological benefits. You will be surprised that it will take you a little bit of intention to find the correct arm to opposite leg coordination at first. This is why I do not recommend walking backwards while holding on to a wall, since you will be preventing normal arm swing. I also advise patients to only walk backwards on the treadmill if they can do it without holding on the the handrails.