While our stated goal is to help people optimize the health potential through our chiropractic invention, the reality is that the majority of people will seek care with their primary focus on addressing pain. Pain is the human experience that is as old as human themselves, and it is a complex topic to put it mildly.
The series is intended to talk about the even more complex subset of chronic pain. Acute onset new trauma related pain is quite different than ongoing chronic pain, from a neurological and physiological perspective. As a result, we need to apply different concepts on addressing chronic pain and acute pain, and quite a bit of the frustration in dealing with chronic pain is that we are trying to apply concepts of acute pain management to a completely different clinical presentation.
1st you need to understand that pain is a brain phenomenon, whether acute or chronic. But the ways in which pain registers in the brain are quite different.
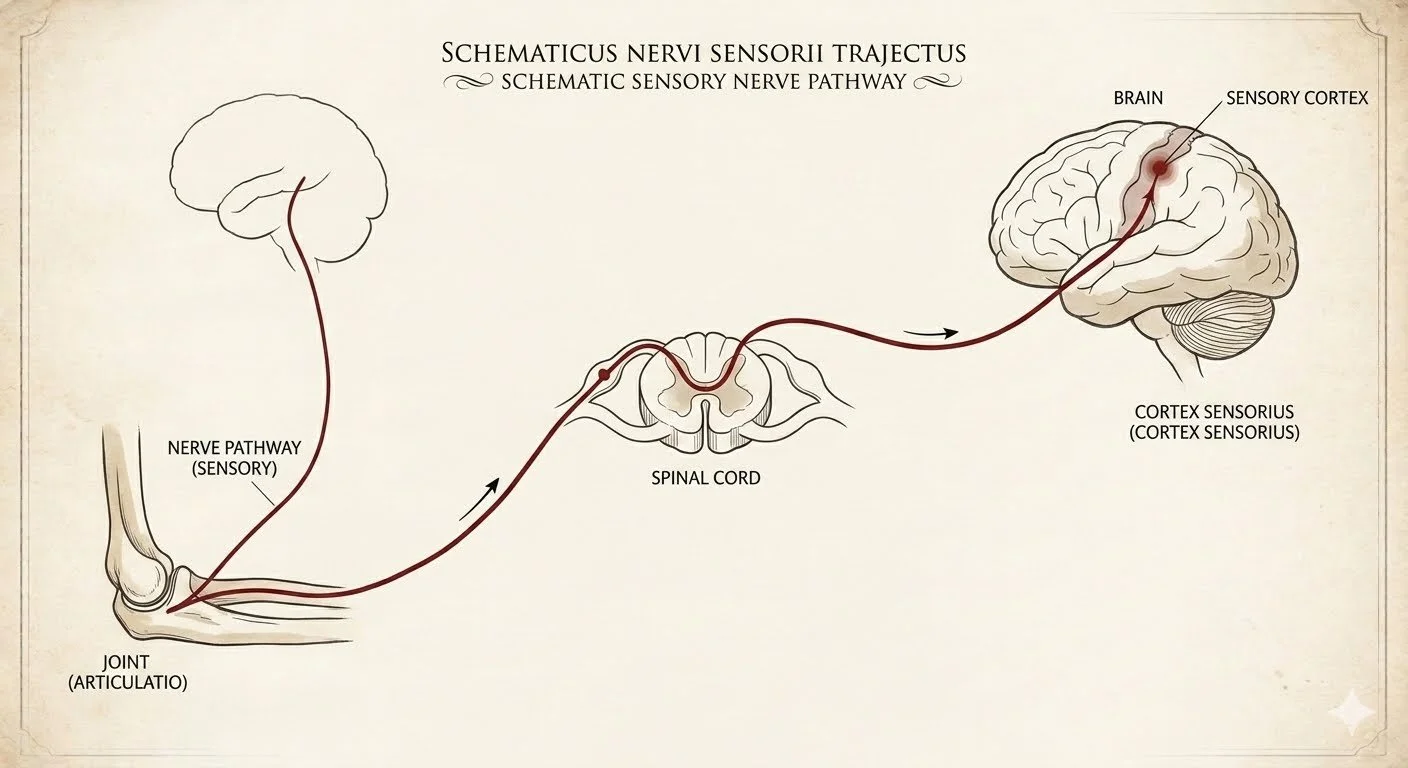
Acute pain: it is mediated through a set of nerves that are large, highly coated in myelin which makes them fast, they have few relay points between the periphery in the brain, and they do not send side branches. As a result, it's pretty much a 1:1 connection between the body insult and the landing place in the central part of the brain cortex. It fires out fast and it turns off equally fast if the periphery receptor is not being activated. To some extent, that's what most people think of as pain, and it's a bit more of an uncomplicated system.
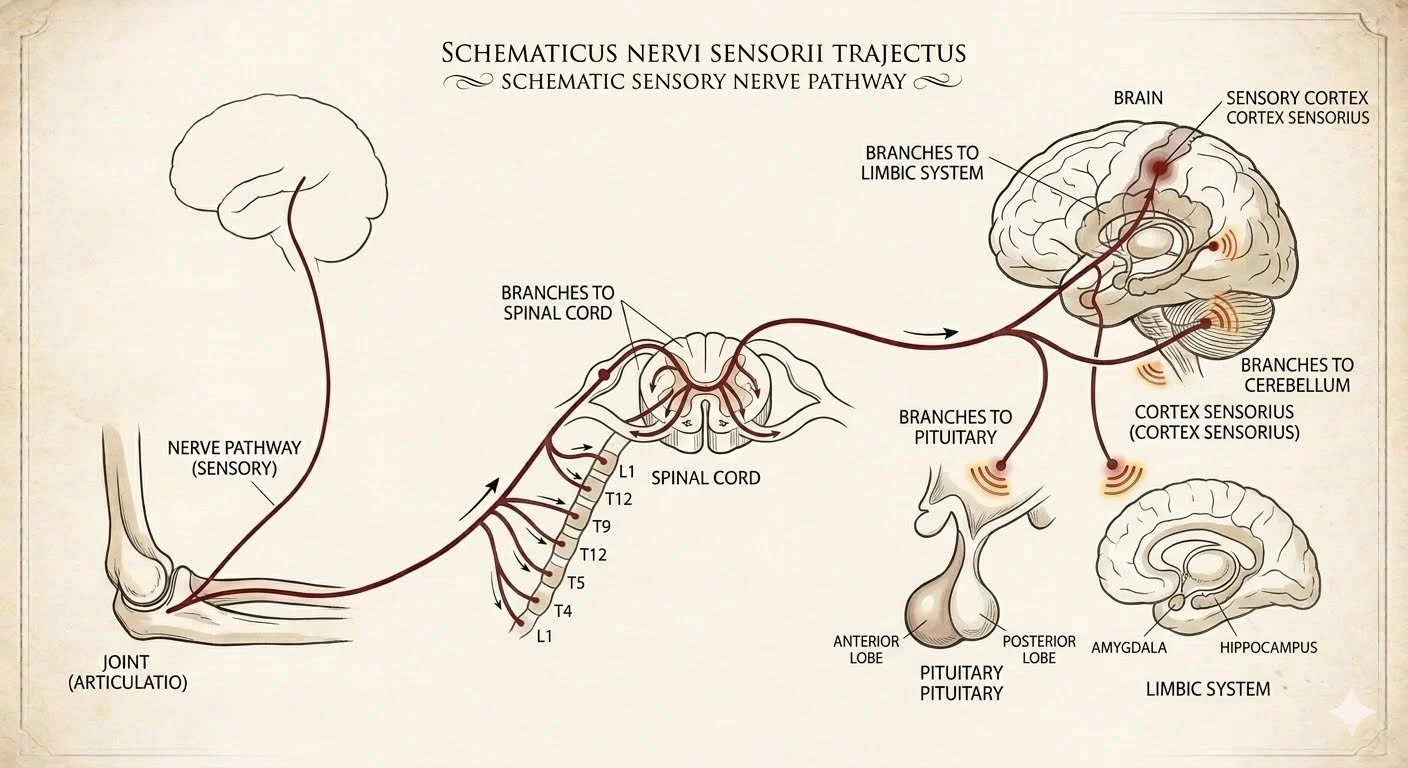
Chronic pain: it looks different neurologically and biochemically. Chronic pain is mediated through a set of fibers that is smaller, slower, and has a lot more peripheral branches, side branches, and spreads to more areas of the brain. The areas of the brain where chronic pain is transmitted are more diffuse, not as well localized in the body, and tend to send connections to part of the brain that are not sensory but associated with autonomic regulations such as mood, sleep and involuntary functions for example digestion and blood flow. It's also highly noteworthy that chronic pain in the brain tends to continuously fire off and be active even if the peripheral tissue from which they originate and not actively being traumatized. As a result, chronic pain can be more uncoupled from the original injury, making it very confusing for the patient to understand why their pain is firing up. The chronic pain circuitry in the brain as well as the small chronic pain fibers are more susceptible to biochemical changes such as inflammation, electrolyte balance, temperature etc.
There is a little bit of a gray area as to when acute pain transitions into chronic pain and why. It's generally accepted that chronic pain pathways can establish as soon as 6 weeks post injury, but in some people it may take up to 3 months. The why question is much more nuanced and will be discussed in a subsequent section.